blog | inmotion training studio

Why "Lift Heavy" Is Only Half the Story: Progressive Overload, Strong Bones, and Protein After 40
Why "Lift Heavy" Is Only Half the Story: Progressive Overload, Strong Bones, and Protein After 40
If you've spent any time in the longevity or fitness world lately, you've heard the advice on repeat: lift heavy. And it's good advice. Strength training is one of the most powerful things you can do for your body, especially as you move through perimenopause, menopause, or — for the men reading — the slow decline of testosterone that comes with age.
But here's what gets lost in the soundbite. When the experts say "lift heavy," most of us can't just walk into the gym and load up a barbell. Most of us are older. Many of us are coming back from injury, time off, or decades of being told cardio was the answer. And if you start heavy before your body is ready, you don't get stronger — you get hurt.
So let's unpack what strength training actually looks like when you're building it intelligently in midlife. We're going to cover progressive overload, why your starting point matters, how your bones get stronger, and why protein and sleep are the non-negotiables underneath all of it.
Progressive Overload: The Real Engine of Strength
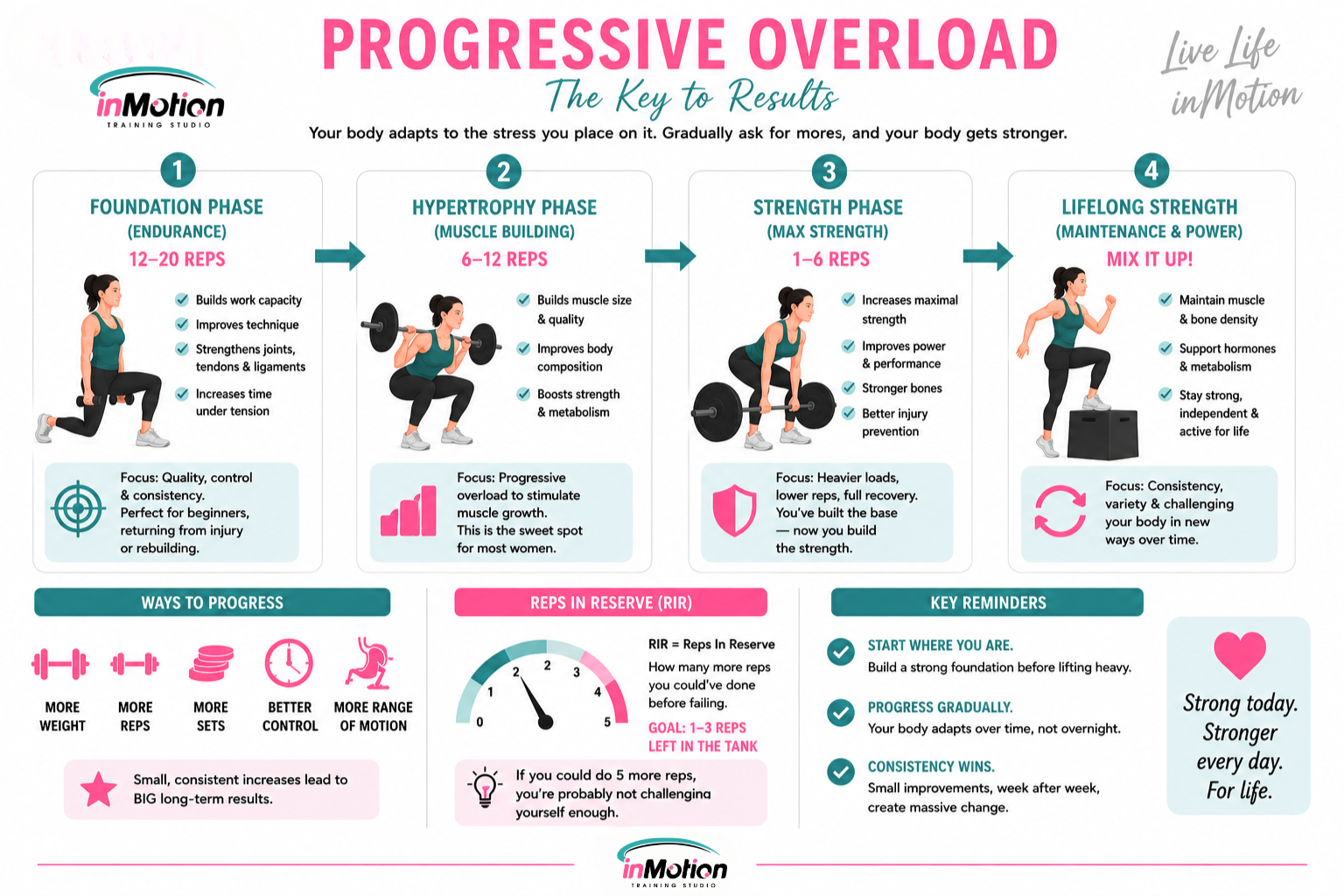
Progressive overload is the single most important principle in strength training. It simply means gradually asking your body to do a little more over time — more weight, more reps, more control, more range of motion. Your muscles and bones adapt to the demand you place on them. No new demand, no new adaptation.
This is the part people skip. They hear "lift heavy" and assume heavy is the starting line. It's not. Heavy is something you earn by progressing toward it. The magic isn't in the weight on day one — it's in the steady, deliberate increase week over week, month over month.
What "heavy" actually means — and why you can't start there
When a 30-year-old athlete is told to lift heavy, their connective tissue, joints, and movement patterns are usually ready to handle it. When a 52-year-old who's been sedentary (or recovering from an injury, or brand new to lifting) is told the same thing, that advice can backfire badly.
Here's why: muscle adapts faster than tendons, ligaments, and joints. You might feel strong enough to add weight before the connective tissue that stabilizes the movement has caught up. Push too hard, too soon, and that mismatch is exactly where injuries happen — and an injury at this stage of life can sideline you for months and undo all your momentum.
So what do you do instead? You build a foundation first.
The phases: where you actually start
Rep ranges aren't just numbers — they tell your body what kind of adaptation you're after. Here's the practical breakdown:
Rep Range Primary Adaptation Who It's For 12–20 reps Muscular endurance, tendon/joint conditioning, technique Beginners, those returning from injury, anyone rebuilding a foundation 6–12 reps Hypertrophy (muscle size and quality) Once your foundation is solid and movement is clean 1–6 reps Maximal strength (true "heavy") Experienced lifters with established technique and tissue tolerance
If you're just starting out, or you've got injuries to work around, you live in that 12–20 rep endurance phase for a while — and that is completely okay. You are not "behind." You're still getting meaningful time under tension, which conditions your muscles, tendons, and joints and teaches your nervous system the movement patterns.
The trade-off is simply that you're not breaking down muscle fibers as quickly or as deeply as you would in a heavier range. You're building the scaffolding. And you need that scaffolding before heavier loading is safe or productive. Rushing past it is how people get hurt and quit.
Once your form is dialed in and your joints tolerate the work, you progress into the hypertrophy range, and eventually — if it's appropriate for you — into true heavy strength work. The path goes endurance → hypertrophy → strength. Not the other way around.
"Reps in reserve": are you actually lifting hard enough?
Here's a gut-check that tells you whether your "heavy" is really heavy: reps in reserve. This is simply how many more reps you could have done at the end of a set before failing. If you finish a set and you had five more reps in the tank, you're carrying five reps in reserve.
And here's the honest truth — if you've got five reps in reserve and you're trying to make progress, you're probably not lifting heavy enough. Your muscles adapt to challenge, and a load you could've repped five more times isn't asking much of them. To drive progressive overload, you generally want to be working close enough to your limit that you've only got one to three reps left in the tank on your working sets.
This is exactly where the caveat lives. If you have an injury or a reason you can't load heavy, listen to your body — staying further from failure is smart and protective, and there's no ego in that. But if you've been training consistently for two to three months, you don't have injuries, or you've recovered from the ones you had and you're feeling better — it's time to start pushing yourself more. Start loading up. A lot of people get comfortable in a weight that stopped challenging them weeks ago, and comfortable is where progress quietly stalls.

Strength Over Cardio — But Don't Skip the Heart
Let me be clear, because this gets misheard too: prioritizing strength does not mean abandoning cardio.
For body composition, bone density, and metabolic health in midlife, strength training should be your priority. But you still need to move your body and elevate your heart rate. The goal is to not let steady-state cardio crowd out your strength work — not to eliminate cardiovascular conditioning altogether.
The good news is you can get real cardiovascular and metabolic benefits from short bursts of higher-intensity effort layered into or around your strength sessions. You don't need an hour on the treadmill to get your heart rate up. Brief, intense efforts give you a lot of return without eating into your recovery or your strength gains.
Building Bone: Osteogenic Loading and the Muscle–Bone Connection
This is one of the most important and least understood pieces of training in menopause — and it deserves real attention.
Muscle–bone crosstalk
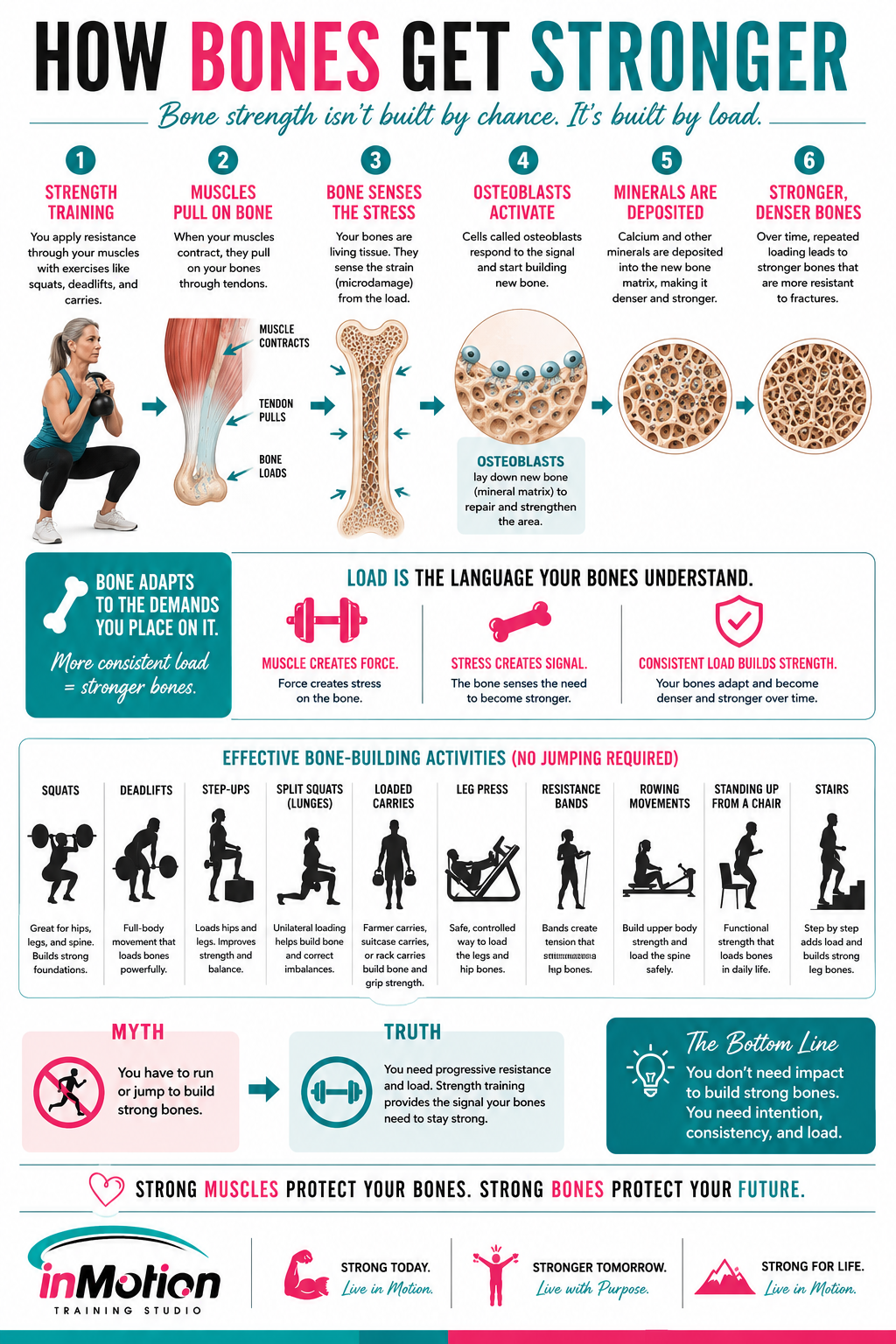
Muscles and bones aren't separate systems. They function as a single unit. When a muscle contracts, it pulls on the tendon, and that tendon pulls on the bone. That mechanical stress — that pull — is the primary signal that tells your osteoblasts (your bone-building cells) to lay down new mineral density.
The lesson here is critical: if you don't have enough muscle mass to create that pull, your bones receive no signal to stay strong. This is exactly why losing muscle in menopause is so dangerous for your skeleton. Less muscle means a weaker signal to your bones, which means accelerating bone loss right at the time estrogen's protective effect is fading. Building muscle is building bone.
Osteogenic loading: bend the bone, build the bone
To stimulate bone growth, you actually want to load the bone enough to bend it slightly. That tiny deformation is the signal that tells your body to deposit more minerals and reinforce the structure. This is osteogenic loading — and it's why heavy, weight-bearing resistance work is so valuable for bone density, far more than any supplement on its own.
Impact and power: the next level (with caveats)
If your body can tolerate it — meaning you don't have a back injury, knee problems, or another contraindication — adding impact is one of the most effective things you can do for bone health. Jumping and high-impact movement create exactly the kind of mechanical stress that drives bone deposition.
This needs to be earned and screened for, not jumped into blindly. But for the right person, low-level plyometrics and impact work are powerful tools. If high impact isn't appropriate for you, weight-bearing resistance training still does the job — you just lean harder on the loading side.
Power and fall prevention
Here's something most bone-health conversations miss: it's not just about strength, it's about power — your ability to move quickly. In menopause, we lose our fast-twitch muscle fibers first. Those are the fibers responsible for quick reactions.
Why does this matter? Because if a client trips, it's her power — that fast muscular reaction — that lets her catch herself before she falls. Improving body composition and training for power directly prevents the falls that lead to fractures. And a higher muscle-to-fat ratio lowers your center of gravity and improves proprioception (your sense of balance), making you genuinely sturdier on your feet.
So we're not just building bones that resist breaking. We're building the strength and reaction speed to avoid the fall in the first place.
Why This Matters More in Perimenopause and Menopause
Estrogen does a lot of quiet, protective work in a woman's body — and as it declines, the things it was protecting start to shift.
In perimenopause (the transition), estrogen and progesterone fluctuate wildly. Cycles get irregular, and "estrogen dominance" symptoms are common. The focus here is symptom management, blood sugar balance, stress and cortisol management, and beginning to build the strength habit. Training is typically strength 2–3x per week alongside restorative movement and a real emphasis on recovery.
In postmenopause (the new normal), estrogen and progesterone settle into consistently low levels. Now the priorities shift hard toward bone density, heart health, insulin sensitivity, and maintaining muscle mass. This is where heavier resistance training, osteogenic loading, and weight-bearing work earn their place.
Estrogen specifically helps with muscle repair, which means it makes the "mechanical loading" from strength training significantly more effective. As it declines, you have to be more intentional — the training, the protein, and the recovery have to do more of the work that hormones used to do for free. This is also where a conversation with a qualified provider about Hormone Therapy can be worth having, since HT (particularly bioidentical hormones) is best understood not as a "fat burner" but as a metabolic stabilizer that supports muscle preservation, bone health, and better sleep.
Protein: The Thing You Prioritize Over Everything Else
If I could get every woman over 40 to change one thing about her nutrition, it would be this: prioritize protein above everything else.
Here's why protein sits at the top of the pyramid:
It's the raw material for muscle repair. Every time you train, you create the demand for tissue to rebuild. Without adequate protein, that rebuild can't fully happen — you do the work and don't capture the reward.
It protects you against muscle loss (sarcopenia). As estrogen declines and age works against you, protein is your primary defense against losing the muscle that signals your bones and drives your metabolism.
It keeps you full and stabilizes blood sugar. High-protein meals improve satiety, which helps manage the "food noise" and cravings that can ramp up in this season.
A practical target many practitioners use is around 1.5 grams of protein per kilogram of body weight per day, distributed across your meals. This becomes especially critical if you're on a GLP-1 medication (like semaglutide), where rapid weight loss can strip away lean muscle right alongside fat if protein and training aren't protected. On those medications, "muscle protection" becomes the entire priority — hit your protein and lift, so your weight loss comes from fat, not from your metabolic engine.
Protein first. Everything else is built on top of it.

Sleep: The Recovery Window You Can't Skip
You can train perfectly and eat enough protein and still stall out if you're not sleeping. Sleep is where the adaptation actually happens, and in midlife it's both more important and harder to come by.
Here's what quality sleep does for your body composition:
Growth hormone release. Roughly 70% of your growth hormone is released during deep sleep — and that's the hormone doing your muscle repair and fat-burning overnight. Short-change your sleep and you short-change your recovery.
It controls cortisol. Poor sleep spikes cortisol and insulin, disrupting your metabolic balance and stress regulation. Chronically elevated cortisol works directly against the body composition you're training for.
It regulates hunger. Just one night of short sleep lowers leptin (the hormone that tells you you're full) and raises ghrelin (the hormone that drives intense hunger for carbs and sugar). You wake up hungrier and reaching for exactly the foods that work against you.
It lowers inflammation. Quality sleep acts as a natural anti-inflammatory, promoting systemic recovery and overall health.
Sleep isn't the "nice to have" at the bottom of the list. It's the foundation that lets the training and the protein actually do their jobs.
Pulling It All Together
If you're newer to this or working around limitations, here's the order of operations:
Start where you are. Live in the 12–20 rep endurance phase if you need to. You're building the foundation, conditioning your joints, and earning the right to go heavier. This is progress, not a holding pattern.
Apply progressive overload. Add a little more over time — that gradual increase is the actual engine of getting stronger. Use reps in reserve as your gauge: if you could've done five more, it's time to load up (unless an injury says otherwise).
Prioritize strength, but keep moving. Don't let steady-state cardio crowd out your lifting; use short bursts for cardiovascular benefit.
Load your bones. Use weight-bearing resistance to bend the bone slightly and signal mineral deposition. Add impact and power work if your body can tolerate it.
Eat your protein. Around 1.5g/kg per day, every day, before you optimize anything else.
Protect your sleep. It's where the recovery, the hormones, and the results actually happen.
Strength training after 40 isn't about ego-lifting or chasing a number. It's about building a body that's strong, sturdy, metabolically resilient, and capable of catching itself when it stumbles — for decades to come.

Shannon / inMotion Training Studio | Live Life inMotion

In motion training studio - bend
social media




REQUEST MORE INFORMATION
change you can do & results you will see


LOCATION
inMotion Training Studio
1279 NE 2nd St, Bend, Oregon 97701